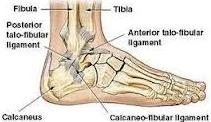
Clinical Features And Treatment of Heel Bone Fracture: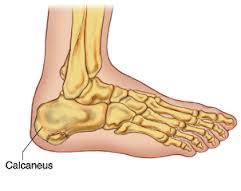 These account for 60 percent of all tarsal injuries and 75 percent of all calcaneal fractures.
These account for 60 percent of all tarsal injuries and 75 percent of all calcaneal fractures.
Mechanism of Injury
Fall From Height: Lateral process of talus acts as a wedge and is forced through the Gissane’s angle resulting in four fracture patterns:
- Undisplaced
- Tongue shaped
- Joint depression
- Comminuted
Clinical Features
Pain and swelling of the heel, the patient is unable to bear weight, stand or walk, pain and difficulty during inversion and eversion of the heel.
Clinical Signs
- Swelling over the heel.
- Tenderness over the heel.
- Lateral heel compression test elicits pain
- Broadening of the heel
- Horseshoe swelling on either side the tendo-Achilles
- Distance between the heel and malleoli is reduced.
Radiography
- Plain X-rays of the foot as in extra-articular fractures.
- CT scan is now emerging as the gold standard in evaluation of intra-articular calcaneal fractures.
Treatment
1) CONSERVATIVE
The following are the basic methods of treatment:
- No reduction and early motion consists
- Elastocrepe bandage application
- Foot elevation
- Weight bearing at the end of 12 weeks
- Closed reduction and fixation.
2) GOALS
Common Steps of Reduction:
- Under anesthesia (general or spinal), the patient is prone and knee is flexed to 90 degree.
- With the assistant supporting the thigh, the surgeon compresses the medial and lateral sides of the heel.
- Strong longitudinal traction is now applied along the direction of the leg.
- Varus or valgus force is now applied depending on the displacement.
- Lastly the calceneal tuberosity is manipulated in position.
- Compression bandage is finally applied.
Surgery
Severely comminuted and depressed fracture with subchondral defects requires open reduction and internal fixation with cancellous bone graft to fill the gap. Recently, for this purpose, alternatively, biocompatible and less re-absorbable nanocrystalline calcium phosphate cement called Bioban is being tried with successful results in some centers. Open reduction and internal fixation with plate and screws are difficult and are rarely adopted.
Complications
- Nonunion is rare due to the cancellous nature of the bone.
- Malunion is more common.
- Heel Pain: The source of heel pain could be from:
- Subtalar joint due to post-traumatic osteoarthritis.
- Peroneal tendonitis due to stenosing.
- Tenovaginitis of the peroneal tendons.
- Bone spurs due to Malunion of fracture.
- Disruption of fat pad of the heel.
- Arthritis of calcaneocuboid joint is a major source of pain.
- Nerve entrapment is rare. Medial or lateral plantar branches of posterior tibial nerve or sural nerve may be entrapped due to soft tissue scarring.
If you are being effected from this fracture come instantly our center Active Physical Therapy. For more information or questions, feel free to contact any of our offices located in Maryland. You can also make your appointment online to start your treatment within 24 to 48 hours at Active Physical Therapy. Call Now at: 301-498-1604
http://www.active-physicaltherapy.com/
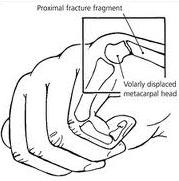
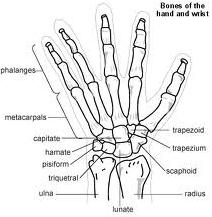 Trapezoid bone injuries are the least typical carpal crack of the hand, including less than 1 % of all carpal bone injuries. Its form and place manage security, and dislocation is probably more typical than crack.
Trapezoid bone injuries are the least typical carpal crack of the hand, including less than 1 % of all carpal bone injuries. Its form and place manage security, and dislocation is probably more typical than crack.